
TO: Director, National Institute for Occupational Safety and Health
TO: Director, National Institute for Occupational Safety and
Health
FROM: Iowa FACE Program
Subject: Silo maintenance worker dies after getting caught in unloading auger -- Iowa.
Summary
 In 1995, a 27-year-old
worker for an agricultural maintenance company was killed while
repairing a silo bottom unloading auger. The victim was working
inside a cement silo filled with corn silage, repairing a sweep
auger that was damaged by frozen feed. The worker was lying on
the silo floor behind the auger safety shield when he shouted
to a workmate outside that he was clear of the auger. The workmate
turned on the auger for approximately 15 seconds to dislodge frozen
corn silage. During this time, the victim apparently reached to
move a trouble light hanging near the auger, and was caught in
the moving auger knives. The victim’s arm and shoulder were
severed, causing severe chest injury. He was taken to a local
hospital and pronounced dead on arrival in the emergency room.
In 1995, a 27-year-old
worker for an agricultural maintenance company was killed while
repairing a silo bottom unloading auger. The victim was working
inside a cement silo filled with corn silage, repairing a sweep
auger that was damaged by frozen feed. The worker was lying on
the silo floor behind the auger safety shield when he shouted
to a workmate outside that he was clear of the auger. The workmate
turned on the auger for approximately 15 seconds to dislodge frozen
corn silage. During this time, the victim apparently reached to
move a trouble light hanging near the auger, and was caught in
the moving auger knives. The victim’s arm and shoulder were
severed, causing severe chest injury. He was taken to a local
hospital and pronounced dead on arrival in the emergency room.
Recommendations following the FACE investigation were:
1. Employers should develop, implement, and enforce a comprehensive written safety program.
2. Employers installing, servicing and repairing silo equipment should provide employee training and proper equipment for confined space entry.
3. Employers and workers should develop a procedure to prevent intentional and unintentional operation of the silo unloading mechanism when a worker is inside a silo or in close proximity to the unloading augers.
Introduction
In 1995, a 27-year-old worker for an agricultural equipment maintenance company was killed while repairing a silo unloading auger. The Iowa FACE Program was notified of the incident by the Iowa Medical Examiners office and began an immediate investigation, followed by a site visit. Information about this incident was obtained from the County Sheriff’s office, newspaper clippings, the medical examiner’s report, an eye-witness statement and interview, the victim’s employer, a farm employee who was present at the scene, and farm owners who had done their own investigation, including the taking of photographs.
The farm had a maintenance contract with a small, out-of-state, agricultural service company which was experienced in silo maintenance and repair. Two employees from this maintenance company were sent to repair a bad bearing and bent end plate of a silo bottom unloading sweep auger. They were an experienced team, working together for 3 ½ years. Their company had been in this business for over 12 years, and at the time of this incident had 5 employees. Written safety procedures did exist for this company, however safety training was not an on-going concern. Each employee had been trained by the owner in safety procedures for working in silos and especially procedures for working with this particular type of silo auger, which is equipped with sharp knives along its entire edge. The presence of these knives often prompts workers to remove V-belts when servicing these augers as an extra precaution against auger movement. Clear systems of communication are vital when working on a silo, especially with one worker inside and another outside operating electric controls. These men had worked together many times and had developed a system of verbal communication, however, they did not follow a lockout/tagout procedure in this case.
Investigation
 The cement silo
is 20 ft. in diameter and 70 ft. tall, used to store corn silage.
Over the winter, the sweep auger had become damaged by frozen
feed inside and needed replacement of the main end bearing and
the end plate. Two employees had begun work on this auger a few
days before, and had returned to finish the job. The victim had
previously entered the silo by removing an access door in its
base and tunneling through some of the silage to provide access
to the end of the auger. The frozen silage was domed over slightly,
allowing only enough room for crawling. The large amount of silage
in the silo was supported only by the frozen edges near the perimeter.
No shoring was done -- the workers relied on the frozen silage
not to fall on them. The victim had hung a trouble light in the
area by wrapping its cord around a large screwdriver and jamming
this into the frozen silage. He was wearing heavy coveralls and
a jacket, as it was a cold day. Oxygen deficiency and the presence
of toxic silo gas were not determined, however it should not have
been a problem as this was the middle of winter, long after the
silo was filled, and the access door had been left open to outside
air for a few days.
The cement silo
is 20 ft. in diameter and 70 ft. tall, used to store corn silage.
Over the winter, the sweep auger had become damaged by frozen
feed inside and needed replacement of the main end bearing and
the end plate. Two employees had begun work on this auger a few
days before, and had returned to finish the job. The victim had
previously entered the silo by removing an access door in its
base and tunneling through some of the silage to provide access
to the end of the auger. The frozen silage was domed over slightly,
allowing only enough room for crawling. The large amount of silage
in the silo was supported only by the frozen edges near the perimeter.
No shoring was done -- the workers relied on the frozen silage
not to fall on them. The victim had hung a trouble light in the
area by wrapping its cord around a large screwdriver and jamming
this into the frozen silage. He was wearing heavy coveralls and
a jacket, as it was a cold day. Oxygen deficiency and the presence
of toxic silo gas were not determined, however it should not have
been a problem as this was the middle of winter, long after the
silo was filled, and the access door had been left open to outside
air for a few days.
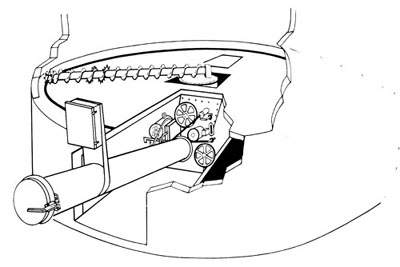
At the time of the accident, the sweep auger was adjacent to the horizontal access door, and the victim was lying behind the auger, on the backside of the sweep, behind the auger shield. The auger was clogged with frozen feed and needed to be cleared before repairs could proceed. The partner was outside, at the opposite side of the silo, next to its electric control panel, preparing to flip the auger switch. He did not have visual contact with the victim who was inside the silo. According to their normal procedures, he asked the victim if he was clear and heard back that he was, then switched on the sweep auger for about 10-15 seconds. A few seconds after the auger was turned off a scream was heard from the victim. He was found in the access tunnel under the silo lying head down on a pile of feed on the floor with his pant leg stuck on a knife of the auger. His left arm and shoulder had been severed and there was extensive injury to his upper chest, and he was complaining of difficulty in breathing.
The county Sheriff and local EMS were called and found easy access to the victim, however he was bleeding badly and was pronounced dead on arrival to the local hospital. The trouble light was not seen at this time, but the co-worker believes it was the only reason that the victim would have reached over the auger shield. He believes it must have been hanging close enough to the auger that the victim tried to move it immediately before or after the auger started. The auger had been repaired, and the silo was operational at the time of our site visit, therefore we did not access the interior of the silo, but made observations from the tunnel under the silo floor.
The exact circumstances of this accident are not known. The victim may have reached for the trouble light; he may have panicked in the narrow space after the auger was turned on; or the auger may have loosened sufficient silage to startle him. Working inside a filled silo is extremely dangerous at any time. The victim thought he was in a safe position behind the auger shield, yet he should have climbed out of the silo, physically away from danger, before his partner turned on the auger. In this type of work a lockout/tagout procedure is required to prevent starting of the auger, intentional or unintentional, while someone is inside the silo.
Cause Of Death
The death certificate listed death caused by massive trauma due to left arm getting caught in power auger. No autopsy was performed.
Recommendations / Discussion
Recommendation #1: Employers should develop, implement, and enforce a comprehensive written safety program.
Discussion: Repairing silo equipment includes several major hazards such as entanglement, oxygen deficiency, silo gas, and entrapment under falling silage. The employers should have a written safety program to address all potential hazards related to silo equipment repair. The employer should ensure that this program is implemented and enforced on job sites, which are commonly on farms far from the employer’s premises.
Recommendation #2: Employers installing, servicing or repairing silo equipment should provide proper employee training and equipment for confined space entry.
Discussion: 29 CFR 1910.272 (g)(6) states "Employees shall not enter bins, silos, or tanks underneath a bridging condition, or where a buildup of grain products on the sides could fall and bury them." Workers should not enter a silo under these hazardous conditions. Employers should provide training and proper equipment for safe confined space entry. Before entry the workers should ensure that the oxygen level is adequate and there are no silo gases present. Secondly they should ensure by shoring that they will not become entrapped under falling silage.
Recommendation #3: Employers and workers should develop a procedure to prevent intentional and unintentional operation of the unloading mechanism when a worker is inside a silo and in close proximity to the unloading augers.
Discussion: The workers should follow a lockout/tagout procedure, disabling the operating controls, when a worker is inside the silo. Starting the auger can cause entanglement and falling of silage. It is highly unsafe to be in the silo while the auger is operating. The lockout/tagout procedure disables the electric controls. Additional protection can be provided by disconnecting V-belts or other mechanical drives to the auger when someone is working inside the silo.
| ___________________________________ | __________________________________ |
| Wayne Johnson, M.D. | Risto Rautiainen, M.Sc.Agr. |
| Trauma Investigator (FACE) | Coordinator |
| Institute for Rural & Environmental Health | Great Plains Center for Agricultural Health |
| University of Iowa -- Iowa City, Iowa | Institute for Rural & Environmental Health |
| University of Iowa -- Iowa City, Iowa |